There is an issue with the cache - please click CTRL + F5 to refresh fully and display correctly. Thank you!
A Covid Treatment Hidden in Plain Sight?
Created on: 2021-10-22
Modified on: 2024-04-30
For a year and a half, we have endured lockdowns, social distancing, mask mandates, travel bans, imprisonment (quarantines), job losses, business closures, increased suicide rates, increased domestic abuse, delays in receiving medical treatment, and much more.
All of this is on the basis that there was no cure for the current pandemic.
Yet from the very beginning, there have been several claimed cures. One of these treatments is vitamin C [VC]. As early as March 2020, Dr Cheng outlined the clinical rationale for this treatment, and referred to the experience already had in China:
High-dose intravenous VC [HDIVC] has also been successfully used in the treatment of 50 moderate to severe COVID-19 patients in China. The doses used varied between 10 g and 20 g per day, given over a period of 8-10 h. Additional VC bolus may be required among patients in critical conditions. The oxygenation index was improving in real time and all the patients eventually cured and were discharged.
So during worst days of the pandemic, the patients in this study, some of whom were in a critical condition, had a 100% survival rate using a protocol including HDIVC. The cohort was small, nonetheless, the results were important. This should have been front page news.
In March 2020, the Expert Group on Clinical Treatment of COVID-19 in Shanghai published its recommendations for treatment, including that:
High doses of vitamin C are intravenously injected 100 to 200 mg/kg per day.
Critics observe that the HDIVC was only one part of the therapy given / recommended in the above. That's true, though the results in the initial study still demand attention.
Another Chinese study was conducted in Wuhan from mid-February to the end of March 2020, to determine the specific role of HDIVC, by giving one group of patients standard care only, and the other, standard care plus HDIVC.
They were unable to recruit their intended number of patients:
". . . the number of qualifying COVID-19 patients decreased with the control of the epidemic so that we had to stop our trial before reaching the predefined sample size."
Also, the treatment was given late in the course of the illness of each patient:
". . . more than 10 days after the first symptom, which may affect the efficacy of HDIVC."
Consequently, the study lacked statistical power, nonetheless, the 28 day mortality in the HDIVC group was half that of the control group. (5 vs. 10.) So, while the study was inconclusive in isolation, the results were promising, prompting further study.
And further study was carried out in Shanghai, and published in April 2021. They looked at past patient records, matching those of patients treated early in the epidemic (mid-January to mid-March 2020) without HDIVC, with similar patients treated later (mid-March to mid-April 2020), who were given the same treatment plus HDIVC soon after the onset of symptoms. They investigated how many patients in each group moved from moderate to severe symptoms:
[A]fter application of the HDVIC protocol since March 23, 2020, fewer . . . patients with moderate COVID-19 on admission evolved to the severe type during the week after admission. These patients also demonstrated [further benefits].
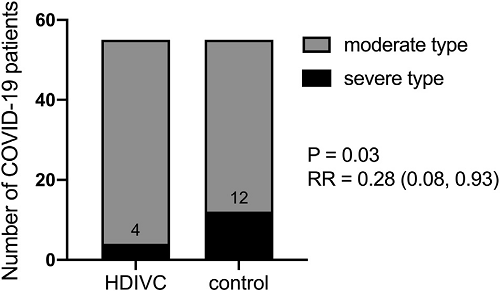
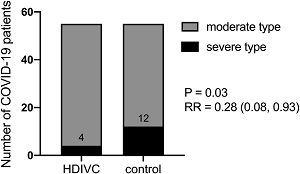
Effect of HDIVC preventing disease aggravation
There were 55 patients in each group; 12 in the control group deteriorated to severe disease, versus 4 in the HDIVC group, a two-thirds drop. While the numbers are small, the difference is so great as to be statistically significant (P = 0.03).
Besides these studies on treatment, there are others that just measured the VC levels in patients.
A study in Barcelona, published in August 2020, found that out of a cohort of 18 COVID patients with ARDS, one patient had low VC, and the remaining 17 (94%) had VC levels so low as to be undetectable.
Another study in Colorado, published in September 2020, looked at vitamin C and D levels in 21 critically ill patients hospitalized in May of that year. Of these, there were 10 deaths. The median age was 61, and the VC levels were low. The authors concluded that:
Older age and low vitamin C level appeared co-dependent risk factors for mortality.
What was the reason for the association between VC levels and disease severity in these studies? Was it cause or effect? It was likely a mixture of both. VC plays an essential role in immunity, and is metabolized in the process of fighting off infections. It is also possible that disease affects absorption of VC through the gut.
In the USA, as early as April 2020, the Front Line COVID-19 Critical Care working group (FLCCC) released the MATH+ protocol,. This includes HDIVC, up to 3g every 6h in the most critical phase of the disease. Again, HDIVC is a part of larger protocol, though at a significantly high dosage. As Mercola summarizes:
The MATH+ treatment grew out of Dr. Paul Marik's vitamin-C-based sepsis protocol, as he and other doctors noticed there were many similarities between sepsis and severe COVID-19 infection, in particular the out-of-control inflammatory cascade.
Various groups that are at higher risk from COVID-19 are also at higher risk of VC deficiency. Older age has been mentioned. Low economic status is another:
Deprivation, while a risk factor for COVID-19 mortality, is also a predictor of low vitamin C status. In the UK, an estimated 25% of men and 16% of women in the low-income/materially deprived population are deficient in vitamin C.
Diabetes and obesity, also risk factors for COVID-19, are also associated with low vitamin C (and D)8.
So there is a strong case for HDIVC, however, orthodox doctors have for decades been divided over its use. This is strange, as the discovery of VC in the 1930s is one of the groundbreaking successes of modern orthodox medicine, and the peer reviewed medical literature supporting it stacks high. However, to many it is simply viewed as alternative medicine.
Resistance to it was clear in the case of Alan Smith, a farmer in New Zealand, who caught swine flu in the pandemic of 2009.
Smith became critically ill; x-rays of his lungs showed them fully whited out. He was put in an induced coma and on an ECMO for survival. After three weeks he showed no progress, and his doctors recommended life support be turned off.
The family objected forcefully that HDIVC be tried before this. Smith's doctors were resistant, but ultimately acquiesced to the family's "strong beliefs in vitamin C," framing it as if it were a tenet of religious faith rather than established science. Nonetheless, after a mere two days of treatment at 25g/day, x-rays showed dramatic improvement in Smith's lungs.
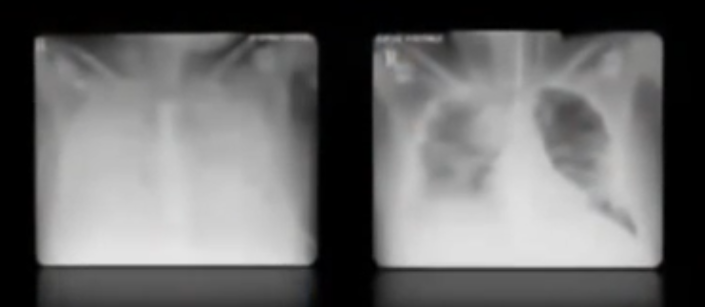
Smith's Lungs, Before and After Two Treatments of HDIVC
However, the doctors had an "out". Prior to giving HDVIC, they proned the patient, turning him face down. This, they claimed, was the reason for his improvement - not the VC.
A child can see through the self-deception. As Smith's family countered - if they were so convinced of the effectiveness of that move, why did they not try that before recommending his life support be turned off?
The saga continued, to and fro, with changes of doctors and treatment, and legal action to force the continued use of VC. Every time the treatment was provided, Smith's condition improved markedly. Every time it was withdrawn, it deteriorated. Ultimately, Smith made a full recovery, from the swine flu and also leukemia. Nobody denied the vital role played by the ECMO and other conventional care. However, the evidence pointing to the VC as making the critical difference between life and death was refuted by his doctors and other commentators. The case is a fascinating lesson not only in medicine, but also psychology.
"The HDIVC group suffered about a fifth of the deaths of the control group, and the odds of this happening by chance alone were less than one in a thousand."
The same prejudice and bias is evident in research material. For example, in 2019, the CITRIS-ALI study was done on HDIVC and patients with sepsis and ARDS - life threatening conditions. Though this was done before COVID-19, it is highly relevant as these conditions are part of the progression of critical COVID-19 cases.
The study of 167 patients concluded:
In this preliminary study of patients with sepsis and ARDS, a 96-hour infusion of vitamin C compared with placebo did not significantly improve organ dysfunction scores or alter markers of inflammation and vascular injury.
In short, it didn't work - they claimed. However, buried within the discussion is this, which you could easily miss:
At day 28, mortality was 46.3% . . . in the placebo group vs 29.8% . . . in the vitamin C group . . . . The Kaplan-Meier survival curves for the 2 groups were significantly different by the Wilcoxon test (chi2 = 6.5; P = .01).
Translation: the treatment group had greater 28 day survival than the control group, (i.e. a greater percentage were alive at day 28) and there is only a 1% chance that this occurred by chance.
The study was reanalyzed; the analysts noted that HDIVC treatment was only given for the first four days and then withdrawn; patients receiving this fared better during this period; when mortality was compared between the two groups at the end of day 4, it was 23% in the control group, and 5% in the HDIVC group. The HDIVC group suffered about a fifth of the deaths of the control group, and the odds of this happening by chance alone were less than one in a thousand.
These are peer reviewed studies in one of the "big four" medical journals - and yet VC is "alternative"? Maybe it is, but not for want of evidence. Proponents of taking VC as a precautionary measure for COVID-19 or for use in hospital protocols such as MATH+ refer to evidence of this nature.
In spite of this, very little use has been made of this in western countries. Current WHO guidance makes no mention of vitamins at all. To some this will be seen as proof that there is no case - though the evidence for it stands.
Self appointed "fact-checkers" have pointed to the "dangers" of VC. The hypocrisy is staggering. At times, the MSM has compared COVID-19 to everything up to the black death, and yet hit pieces warn us that too much VC could cause some minor problems. The reality is, VC is very safe.
Conclusion
Studies on the effectiveness of HDIVC as a treatment for COVID-19 have shown significant results, and in some parts of the world it has become part of standard treatment. Decades of medical literature shows the effectiveness of VC against all viral illnesses researched, and some of the more dangerous conditions associated with COVID-19. Low VC levels correlate with comorbidities and other factors associated with higher risk from COVID-19. Studies on critically ill COVID-19 patients have shown low to undetectable VC levels.
As ever, this is not medical advice, though common sense tells us that if we are in any high risk groups that we can change, we should fix that, as a precaution. Many people took the current situation as the prompt to fix problems with their health, such as obesity.
HDIVC, MATH+ and the like would require a hospital or at least a doctor to administer, and are suited only to care, not prevention. What can we do for ourselves? Again, not medical advice, but oral supplementation of VC can ensure our levels remain healthy, to fortify our immune systems.
From March 2020, many of us in the natural health sector didn't wait for any more studies. We anticipated, based on decades of medical research and experience, that VC would be important, and therefore many of us started, or restarted supplementing VC as a precaution.
I don't recommend panic buying - instead, always be in stock. Nonetheless, as a result of the current situation, suppliers to the natural health sector were for a time cleaned out of vitamin C in March 2020, such was the awareness in the natural health sector of the importance of this vitamin. Conventional care in the West has for the most part yet to catch up.
- Antony
Notes
: See also Hydroxychloroquine.
: Cheng, et al., Can early and high intravenous dose of vitamin C prevent and treat coronavirus disease 2019 (COVID-19)?, Med in Drug Discov, 2020 Mar 5
: Shanghai new coronavirus disease clinical treatment expert group, Shanghai 2019 coronavirus disease comprehensive treatment expert consensus, Journal of Infectious Diseases, 2020 Mar 3, translation provided by Anderson using MS-Translate
: Zhang, et al., High-dose vitamin C infusion for the treatment of critically ill COVID-19, Research Square [preprint], 2020 Aug 10
: Zhao, et al. High Dose Intravenous Vitamin C for Preventing The Disease Aggravation of Moderate COVID-19 Pneumonia. A Retrospective Propensity Matched Before-After Study, Front Pharmacol, 2021, Apr 21
: Chiscano-Camón, et al., Vitamin C levels in patients with SARS-CoV- 2-associated acute respiratory distress syndrome, Critical Care, 2020 Aug 26
: Acute Respiratory Distress Syndrome
: Arvinte, et al., Serum Levels of Vitamin C and Vitamin D in a Cohort of Critically Ill COVID-19 Patients of a North American Community Hospital Intensive Care Unit in May 2020: A Pilot Study, Med in Drug Discov, 2020 Sep 18
: MATH+ Protocol, updated since original publication.
: Marik, et al., MATH+ protocol for the treatment of SARS-CoV-2 infection: the scientific rationale, Expert Review of Anti-infective Therapy, 2020 Aug 18
: Mercola, et al., The Truth About COVID-19, 2021
: Holford, et al., Vitamin C—An Adjunctive Therapy for Respiratory Infection, Sepsis and COVID-19, Nutrients, 2020 Dec 7
: Levy, Curing the Incurable, 2011
: Vitamin C The Miracle Cure 60 Minutes Living Proof
: Fowler, et al., Effect of Vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients With Sepsis and Severe Acute Respiratory Failure, The CITRIS-ALI Randomized Clinical Trial, JAMA, 2019 Oct 1
: Hemilä, et al., Reanalysis of the Effect of Vitamin C on Mortality in the CITRIS-ALI Trial: Important Findings Dismissed in the Trial Report, Front Med, 2019 Oct 7
: COVID-19 Clinical management: living guidance, WHO, 2021 Jan 25
Notify me of new posts:
For help with health, see here.
Latest Post:Update from Healing TruthsWhere I've been for the last year. Two schools of thought in natural healing. 23 Apr '26 | Next Post:Waning Vaccine EffectivenessCOVID vaccines have been claimed to be 90-100% effective. However, these claims are disputed even by orthodox medical sources. 11 Nov '21 | Previous Post:Deadly Dermatology versus Collateral HealingA suicide linked to an orthodox acne drug has recently been in the UK news. But alongside the risk of death are many other side effects, and limitations of the pharma approach. What does alternative healing have to offer instead? 7 Oct '21 |
Latest Post:
Update from Healing Truths
Where I've been for the last year.
Two schools of thought in natural healing.
23 Apr '26
Next Post:
Waning Vaccine Effectiveness
COVID vaccines have been claimed to be 90-100% effective. However, these claims are disputed even by orthodox medical sources.
11 Nov '21
Previous Post:
Deadly Dermatology versus Collateral Healing
A suicide linked to an orthodox acne drug has recently been in the UK news. But alongside the risk of death are many other side effects, and limitations of the pharma approach. What does alternative healing have to offer instead?
7 Oct '21